RNY to DS vs. RNY to BPD in plain English is there a difference?
on 12/15/09 10:38 am - Tampa, FL
What were some of the differences they mentioned to you?

This article was just posted on the same subject:
www.obesityhelp.com/forums/Revision/4083209/Considering-ERNY -revision-May-want-to-look-at-inside-link/
I got a revision from a 1980 gastric bypass and am thrilled with the results, it's wonderful to have my pyloric valve and duodenum back. No way I would settle for ERNY or BPD.
Kerry


Who were the surgeons?
If I was going to revise from RNY to anything it would be the DS. I would also make sure that I talked to the big gun revision surgeons - Greenbaum and Rabkin, come to mind - I am sure there are other ones out there that I can't think of now. I would also make sure that they take down the pouch and give you a fully functioning VSG tummy and do the switch on the intestines.


on 12/15/09 10:55 am
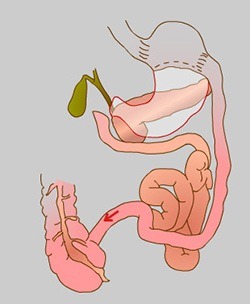
The top picture is the BPD or Scopinaro procedure, not really the original BPD, Scopinaro said he improved the original BPD. http://www.keyholesurgerycentre.com.au/pancreaticd.html

The bottom picture is the Duodenal Switch. The difference is in the stomach.
The main reason I can see to pick the BPD would be if your remnant stomach is atrophied and your pyloric valve will not re-activate, if that is the case you would really have no choice. Another reason might be the incidence of leaks when they take down the RNY pouch and re fashion the stomach, then they have to cut the stomach to make the sleeve.
I cannot advise you as I don't know which surgeons you have talked to. I can tell you that I would only have the very best to perform either one of those surgeries.
HTH,
Michele

Red

There are some surgeons who are recommending this sort of hybrid operation instead of a true RNY to DS revision. There are any number of names for it, but it boils down to a variant of the ERNY. It's true that it's less risky than a full RNY to DS conversion, which is a very complex operation. However, it preserves the RNY pouch with it's connection to the small intestine. Thus, whatever problems you have with your pouch - dumping, stretched out stoma with insufficient restriction, food getting stuck, whatever - you would still have with this "BPD - like" operation (as one surgeon calls it).
In addition, you would have malabsorption similar to the DS. While this might promote some weight loss (no one really has longterm statistics for this thing), it would give you the vitamin and protein malabsorption of the DS, but without the fully functional sleeve stomach that we have to get in extra protein and nutrients. AND you would keep the calcium and iron issues of the RNY as the entire duodenum would still be bypassed.
While a true conversion to the DS would carry more initial risk, I believe it would be superior in the long run both for weight loss and for nutrition. Also, even though your stomach hasn't been in use for awhile, what I've heard from surgeons who do RNY to DS is that the function gradually returns. In other words, a non-functional sleeve isn't what they are seeing post-op.
Only you can decide how much risk is acceptable to you.
Please feel free to pm me for more info - Red sent me!
Larra
on 12/15/09 4:56 pm
The BPD is the old version of the DS - it was called the BPD with Duodenal Switch. It involved making a larger pouch than with the RNY and completely removing the remnant stomach (with the RNY, the remainder of the stomach is left inside the patient). The common channel was then made somewhat shorter than with the modern DS surgery. It was pioneered by Dr. Scopinaro in Italy. It is not done anymore because so many patients had serious vitamin/mineral deficiencies, metabolic and bowel problems. It is the "grandfather" of the modern DS.
The modern DS involves making the stomach into a "sleeve", not a pouch. You would not have the stoma of the RNY - your anatomy would be more "natural" because your pyloric valve would be back in charge instead of the "man-made" stoma (these can stretch out). Also, the greater curvature of your stomach would be completely removed - this is important because this is where the majority of the hunger hormone, Grehlin is produced. This helps enhance the metabolic effect of the DS surgery.
The doctor who is suggesting that you leave the pouch alone and just do the "switch" probably doesn't have the skill to do the entire surgery as a revision (even though he/she might do the virgin DS on a new patient). You need to find out if this doctor would be removing your blind stomach, thereby making you unable to EVER convert to the full DS (because you won't have enough stomach to cut into a sleeve), or if he/she would be leaving it still in you. If your blind stomach is still left in you, you would probably have a version of the ERNY (Extended RNY - also sometimes called distal or very long limbed RNY). If it is removed, you would be left with a form of the old Scopinaro procedure.
From everything I've read on these boards, the full DS revision is more effective in both losing more excess weight and keeping the excess weight off than the ERNY. The DS also has important differences in the ways the intestines are re-arranged, so that there are less malabsorption problems than with the ERNY. Dr. Keshishian (one of the DS surgeons) was recently posting on either the DS or revisions board discussing this and answering questions.
Best of luck with whichever procedure you choose.
The BPD is the old version of the DS - it was called the BPD with Duodenal Switch.
The surgery being done today and what we call the duodenal switch for short is many times called the bilipancreatic diversion with duodenal switch (BPD/DS). The old surgery is called the biliopancreatic diversion (sometimes with Scopinaro method tacked onto the end).
Red

Valerie
DS 2005
There is room on this earth for all of God's creatures..
next to the mashed potatoes
![]()

