Looking into revision from a VBG...

I had a VBG in 2001, with a starting weight of 351lbs. I lost 125lbs in about 13 months, and then got pregnant way too soon. After the birth of my son, my weight started creeping back up - I've been dieting on and off since 2003.
I'm at the point now where I'm almost back to my "starting" weight - I weighed in today at the dr's at 339lbs. :( I'm having a lot of pain in my stomach and back these days, and on Thursday of next week I have to go for an Upper GI series so we can see what's going on in there.
I'm so frustrated! I have no idea how long this process will take, if I'll even be approved, which surgery is "right" for a revision, etc.
I guess I'm just looking to hear how others have done, and that there might actually be light at the end of this tunnel - one that's NOT a train, LOL.
Thanks.
Tabatha
Referral to Surgeon: February 12, 2013 Appointment with Surgeon: April 24, 2013 Endoscopy: April 30, 2013 Referral sent to Bariatric Registry: May 2, 2013 Orientation Appointment: May 27, 2013 Dr Klein Appointment: June 6, 2013 Second Upper GI Series: June 11 Dr Glazer: August 12, 2013 RN/RD/SW: August 29. 2013 Follow-up With Dr Klein: September 23, 2013 Start Opti: October 23, 2013 Surgery Date: November 14, 2013


on 9/21/12 7:17 pm
The thing is, you can go to any surgeon, and I assure you they will recommend a procedure they do, regardless of whether or not it's best for you. The other issue is that while the DS is the most successful weight loss surgery, there are only a few surgeons that will do the revision to it.
You can find links to most of the studies and articles and lots of other useful information at DSfacts.com, as well as a list of vetted surgeons.
From your standpoint, why is the DS better than the RNY or Sleeve?
Again, thanks for your response. :)
Referral to Surgeon: February 12, 2013 Appointment with Surgeon: April 24, 2013 Endoscopy: April 30, 2013 Referral sent to Bariatric Registry: May 2, 2013 Orientation Appointment: May 27, 2013 Dr Klein Appointment: June 6, 2013 Second Upper GI Series: June 11 Dr Glazer: August 12, 2013 RN/RD/SW: August 29. 2013 Follow-up With Dr Klein: September 23, 2013 Start Opti: October 23, 2013 Surgery Date: November 14, 2013
on 9/24/12 8:48 am
From your standpoint, why is the DS better than the RNY or Sleeve?
Again, thanks for your response. :)
Many of the reasons I don't like RNY is that the pylorus is cut from the bottom of the stomach, and then you are given a man made "stoma" for food to exit the stomach, and that is the root of many of the RNY issues. Having intestinal tissue attached directly to the stomach can be problematic as it's not designed to withstand stomach acid, and can get ulcers. The stoma is also prone to getting too tight from scar tissue, and more commonly (and more problematic) is the stoma stretching and becoming too large, which allows food to dump too quickly into the intestines, while not being adequately digested. This is the root for RNY issues like dumping, and reactive hypoglycemia, and possibly weight regain due to the stomach emptying too quickly. The procedures that have been tried for re-tightening the stoma like Rose and stomaphyx, have not been successful.
With RNY, the stomach portion that is not used to make the pouch, is left in the body, which can also create problems. It's possible to get ulcers, or cancer in the unused stomach, but it can't be scoped to see those things. With RNY, you also cannot ever take NSAIDs for pain, which was a big deal for me.
Finally, I just didn't like the success rates for anything but the DS. I needed to get a lot of weight off, and keep it off. It wasn't worth doing if it was just a minor or temporary fix. Surgery is a big deal to me, and I only wanted to go through it once. Again, I highly recommend looking at the studies at the site I mentioned before, as they give alot of information about the different surgeries.
The IS a surgeon there that does the DS, and I know others who wanted the DS asked to be referred to him, but I can't recall his name. I suggest asking on the DS board who he is, and how others managed to get hooked up with him.
Referral to Surgeon: February 12, 2013 Appointment with Surgeon: April 24, 2013 Endoscopy: April 30, 2013 Referral sent to Bariatric Registry: May 2, 2013 Orientation Appointment: May 27, 2013 Dr Klein Appointment: June 6, 2013 Second Upper GI Series: June 11 Dr Glazer: August 12, 2013 RN/RD/SW: August 29. 2013 Follow-up With Dr Klein: September 23, 2013 Start Opti: October 23, 2013 Surgery Date: November 14, 2013
on 9/22/12 4:08 am
So start looking for a DR and get testing done and find out what went wrong. He said he would remove most of my stomach like a sleeve, but i would only have a square portion and then do a bypass.
Good luck to you and keep us posted
My biggest concern is what options are available to me as far as revisions. My GP thinks VSG, but I've heard better things about the bypass. I've tried to do as much reading/research as I can, but I'm not able to find much on revisions.
It sounds like you're on the right track - I don't envy anyone who has to deal with insurance issues. :( I'll have my fingers crossed for you!

Sorry, I'm such a newbie with this stuff. When I had the VBG it was the ONLY option available, so I didn't go as research-crazy as I'm going this time.
Referral to Surgeon: February 12, 2013 Appointment with Surgeon: April 24, 2013 Endoscopy: April 30, 2013 Referral sent to Bariatric Registry: May 2, 2013 Orientation Appointment: May 27, 2013 Dr Klein Appointment: June 6, 2013 Second Upper GI Series: June 11 Dr Glazer: August 12, 2013 RN/RD/SW: August 29. 2013 Follow-up With Dr Klein: September 23, 2013 Start Opti: October 23, 2013 Surgery Date: November 14, 2013

And, just to be thorough, here's a pic of the DS:

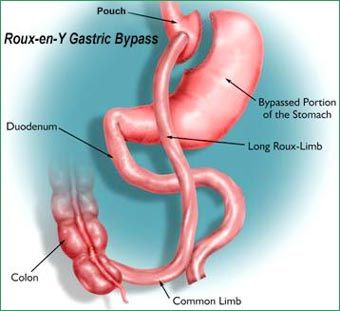
The RNY cuts the stomach into a tiny pouch that holds food, and a huge, 'blind' remnant stomach that just---hangs out. (*grin*) The pouch has a stoma, or a man-made, always-open, hole poked into it that allows food to pass into the small intestine, and a small amount of the small intestine is bypassed to give some malabsorption. Unfortunately, this causes permanent malabsorption of certain vitamins and minerals, but only temporary malabsorption of calories, the things that give most of us trouble.
The Sleeve, on the other hand, removes around 90% of the stomach---removes it completely from the body, where it can never bother us again. It's not like the remnant stomach of th RNY, just hanging around and producing ghrelin, the 'hunger hormone', or potentially getting ulcers, developing fistulas, etc. It's simply a MUCH smaller, yet fully-fucntional stomach.
The DS has roughly the same stomach as the Sleeve, plus an intestine bypass similar to, but more agressive than, the RNY. This more aggressive intestinal bypass still causes permanent malabsorption of certain vitamins and minerals, but it also causes permanent malabsorption of calories, too. This is why the DS has the very best long-term, maintained weight-loss stats.
To my way of thinking, the RNY has more potential problems than benefits, when compared to either the Sleeve or the DS.



