Post Roux-en-Y Scopionara BPD

On June 22, 2011 at 3:10 PM Pacific Time, Peter F. wrote:
Hi Guys,Had RNY about 10 yrs ago with a BMI of 60 went down to a BMI of 40 and am now back to a BMI of 50. Is this common? Saw a surgeon who suggested a "Post Roux-en-Y Scopionara BPD" any-one had this done and any comments and advice would be appreciated.
www.dssurgery.com/about/publications/duodenal-switch-safe-op eration.pdf
On June 23, 2011 at 2:38 AM Pacific Time, Peter F. wrote:
unfortunately don't reside in USA so have to go with the local surgeon. Do you know anything about this specific procedure?
did Dr Gagner do your RNY? he is the first sugeon to do the lap DS, I am confused he is the one that recommended the BPD? that does not sound like him at all, he is very pro VSG and DS, very few surgeons do the BPD, and you want to perserve your pyloric valve. ask the surgeon exactly what s/he will do and get the specifics...good luck on your revision
Gagnier did the RNY although he said that the DS was the most appropriate procedure but he was concerned abou the lack of post-operative monitoring and support when I returned home to South Africa. It is the SA bariatric surgeon who said that as I already have the RNY pouch, the Scarpinaro BPD is the way to go. Also he prefers to do it as open rather than laparascopically. Any thoughts?

Here are some visual aids:

A true DS (sometimes called a BPD with DS/duodenal switch) looks like this:
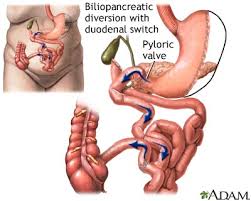
The top pic is of a Scopinaro BPD. AS you can see, it's basically a large-pouch, extremely-distal version of what you have now. It's a pretty effective procedure, as far as weight loss is concerned, but it has some serious drawbacks re vitamin deficiencies and bowel issues.
When Dr. Hess developed the DS, out of respect for the pioneering work Scopinaro did with the BPD, he called it the BPD-DS---which is a really misleading name. It really should be called the VSG-DS (Vertical Sleeve Gastrectomy with Duodenal Switch), because a true DS does not have a pouch and stoma---in fact, replacing the pouch and stoma with a fully-functional stomach is the major reason the DS is considered an improvement over the old BPD.
If at ALL possible, I urge you to go back to Gagner and get a true DS. It will give you a better quality of life than the BPD will, and will NOT require any more post-op monitoring and support than the BPD would.
Revising from the RNY to a true DS requires a VERY skilled surgeon. The SA surgeon you're seeing may not feel competent to do the necessary stomach revision, and/or to sew the duodenum---I've heard it compared to sewing wet tissue paper. Gagner CAN do this, and frequently does.

A true DS (sometimes called a BPD with DS/duodenal switch) looks like this:

The top pic is of a Scopinaro BPD. AS you can see, it's basically a large-pouch, extremely-distal version of what you have now. It's a pretty effective procedure, as far as weight loss is concerned, but it has some serious drawbacks re vitamin deficiencies and bowel issues.
When Dr. Hess developed the DS, out of respect for the pioneering work Scopinaro did with the BPD, he called it the BPD-DS---which is a really misleading name. It really should be called the VSG-DS (Vertical Sleeve Gastrectomy with Duodenal Switch), because a true DS does not have a pouch and stoma---in fact, replacing the pouch and stoma with a fully-functional stomach is the major reason the DS is considered an improvement over the old BPD.
If at ALL possible, I urge you to go back to Gagner and get a true DS. It will give you a better quality of life than the BPD will, and will NOT require any more post-op monitoring and support than the BPD would.
Revising from the RNY to a true DS requires a VERY skilled surgeon. The SA surgeon you're seeing may not feel competent to do the necessary stomach revision, and/or to sew the duodenum---I've heard it compared to sewing wet tissue paper. Gagner CAN do this, and frequently does.


Most Active
Recent Topics



