 email to a friend
email to a friend printer-friendly version
printer-friendly version| Body Contouring as an Outpatient Procedure - Plastic Surgery by Robert Ersek, MD, FACS, with Nicole Chambless, BA; Peter Chang, MD; Mark Salisbury, MD; and Inna Wilkerson, MD - May 2007 In recent years, gastric bypass and a variety of dietary and exercise regimens have resulted in many patients losing more than 100 pounds. The patients are left with loose hanging skin. Often, the psychological results of obesity may be more apparent than ever, resulting in a diminished quality of life. Through a variety of body contouring procedures that are safely performed on an outpatient basis, we are able to remove the stigma that massive weight loss causes in these patients. Materials and Methods Bariatric patients are encouraged to achieve their maximum weight loss goals prior to any surgical body contouring procedures. On average, this occurs somewhere around 17 months post-surgery. We outline a program which will include a variety of procedures, including abdominoplasty (tummy tuck), breast lift, brachioplasty (arm lift), thigh lift, hip lift, facelift, blepharoplasty (eyelid surgery), brow lift, and saddle lift. We may perform these procedures sequentially based on the individual?s recovery time, work schedule and budget. In most cases we do some liposuction to remove weight loss-resistant bulges of fat. These areas most often include the flanks, calves and arms. We do not perform liposuction in an area that is to have open surgery at the same time. This staging is important because in areas where blunt liposuction is applied, large lymphatic drainage pools will form that will usually heal quite well. However, if the adjacent area is undermined, as in abdominoplasty, a pseudo bursa (scar-lined pocket) may form, possibly requiring another operation. To completely avoid this situation, suction and surgery should be performed separately, allowing 6 weeks between each procedure. For very large cases we require that patients donate one or two units of their own whole blood a few weeks prior to surgery. We give the patient the blood at the end of the procedure whether or not they ?need? it physiologically. After liposuction, we plan and then perform the combination of procedures that are appropriate to the patient in two, three, or four sessions. We perform liposuction first, in order to achieve maximum results before creating any addition scarring. Anesthesia All of these outpatient procedures are performed under Valium and ketamine dissociative anesthesia. We then infiltrate the entire area that is to be treated with Xylocaine with epinephrine and Ringer?s lactate solution. This usually takes 10 to 15 minutes to complete and the patient is completely anesthetized; their reflexes, muscle tone and respiration, however, remain intact. This infiltration provides local anesthesia to the entire area to be treated. The epinephrine and fluid cause very little blood to be present in the fat that is extracted. During the procedure, if it takes more than one to two hours, a subsequent addition of Valium or ketamine may be administered. We are able to record and evaluate the amounts and timing of medications with a sedation monitor (SeMo®) device we have developed. The SeMo indicates the medications, duration of activity and the amount given. This makes it very simple to see at a glance exactly what was given and when. The SeMo prints out a color record for the patient?s chart at the end of the case, so we are able to avoid the troubles of flipping through a chart or trying to decipher someone?s handwriting. Closure In skin-removal operations (dermalipectomies) bleeding is controlled with electrocautery. In the case of an abdominoplasty, several layers of internal or external oblique muscle or the Linea Alba may be used to create an internal corset when necessary. All of our incisions are closed with absorbable sutures and a running subcuticular stitch reinforced with suture strips. No staples or skin stitches are ever used, leaving our resulting scars minimal with no signs of cross hatches or railroad tracks. 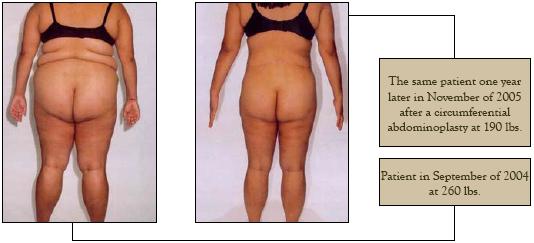 Results Our patients are given the option to have a complete body overhaul performed on their schedule with a minimum of downtime because of careful staging of the operations. Every patient either returns home, goes to a hotel, or is sent to a special care facility that night where they will remain for the next few days. In most cases, our patients are able to return to work in less than one week. In the case of abdominoplasty, our patients have drains that are removed approximately three days postoperatively, depending on their individual drainage. During the past 10 years, we have performed these procedures on 847 patients. Nearly all of our patients are treated as outpatient procedures in our facility. In our experience, a patient who is hospitalized will accrue two to three times the amount of charges as an outpatient in our facility for the same procedure. In our facility we find less morbidity, mortality, and liability for our patients.  In thirty years, using these methods for all cosmetic and reconstructive surgeries we have never had a deep vein thrombosis, pulmonary embolism, vocal cord injury, aspiration, arrhythmia, chipped tooth, positive pressure pneumothorax, a negative-pressure pulmonary edema, arrest or mortality, or awakening of paralyzed patient, all of which are reported with general anesthesia and incubation. In our own practice, the majority of the complications seen in patients post-operatively have been the occurrence of slow healing wounds and poor circulation. We have had two cases of abdominal skin loss in massive abdominoplasty procedures in conjunction with poor circulation. In both cases, these patients continued to smoke despite our warnings.  The Big Picture  A complete body makeover can be accomplished safely as an outpatient procedure. A study at Johns Hopkins states that ?patients requiring surgical skin excision after massive weight loss for functional or aesthetic reasons are challenging, and require individualized approaches?? We are able to perform the necessary procedures in a scheduled manner over period of months, requiring minimal downtime while avoiding many of the more common complications with the use of Valium, ketamine dissociative anesthesia and outpatient facilities. The result of post-bariatric body contouring using dissociative anesthesia is a low complication rate, a timely recovery, and high patient satisfaction. In addition to the luxury of being treated as an outpatient under dissociative anesthesia, our patients notice significant cost reductions. Because we are able to exactly calculate our costs, there are no hidden hospital fees. Our surgical clinic is on site, so there is no hospital fee. We do not use a general anesthesia, so there is no fee for an anesthesiologist. Our fees are global and cover operating and recovery rooms, anesthesia, surgical fees, our standard lab work and pre-op and post-op care. Our patients are able to accurately budget all expenses prior to their surgery date.  Robert A. Ersek, MD, FACS, was an early adapter of the liposuction techniques that were first introduced by Girard Illouz of Paris in 1983. He has published extensively and has substantial experience teaching world wide as a traveling professor for the International Society of Aesthetic Plastic Surgeons. He is currently President of the International Society of Clinical Plastic Surgeons and Dean of the Lipoplasty University. His clinic, Personique, performs all procedures on an outpatient basis under Valium and ketamine dissociative anesthesia. For more information, please visit www.plasticsurgeryexperts.com or call 888-737-7664. Robert A. Ersek, MD, FACS, was an early adapter of the liposuction techniques that were first introduced by Girard Illouz of Paris in 1983. He has published extensively and has substantial experience teaching world wide as a traveling professor for the International Society of Aesthetic Plastic Surgeons. He is currently President of the International Society of Clinical Plastic Surgeons and Dean of the Lipoplasty University. His clinic, Personique, performs all procedures on an outpatient basis under Valium and ketamine dissociative anesthesia. For more information, please visit www.plasticsurgeryexperts.com or call 888-737-7664.Want to learn more about plastic surgery? Visit the Plastic Surgery Forum Homepage or check out the Plastic Surgery Message Board. |
Most Active
Recent Topics

Seeking exceptional California plastic surgeon for breast implants!
donnaloza · 1 replies · 105 views
donnaloza · 1 replies · 105 views

