Researching the Sleeve? Early and Late leaks CAN and DO happen

on 5/1/13 11:41 pm, edited 5/2/13 1:04 am
Again, there are many lap banders that are considering the Sleeve, if they have to get their bands removed. Leaks rates are MUCH HIGHER with band to Sleeve revisions than virgin Sleeves and hard to treat and manage, which can debilitate the patient or be deadly.
Knowledge is power, I know sometimes we are desperate for a quick fix and we all hope for a "perfect wls" but that does not exist.
They first said the Sleeve did not stretch, they first said Leaks can only happen the first few months post op, but that is NOT true, leaks CAN HAPPEN ANYTIME with the Sleeve, there can be a break in the Staple.....many months/years post op.
I think those who are pushing the Sleeve and DS are down playing LONG TERM issues with both surgeries, not sure why. They also down play hypoglycemia which can be deadly and debilitating....Reflux/and horrible heartburn is the least of your worries....
Stretching is inevitable regardless of how well the Sleeve is done, there are many studies to back that up also...
Long term leak study...
More links on Late Leaks
http://www.bmilatina.com/index.php/bmi/article/view/8
http://bariatrictimes.com/endoscopic-management-of-persistent-leak-after-laparoscopic- sleeve-gastrectomy-a-case-report/
Endoscopic Management of Persistent Leak after Laparoscopic Sleeve Gastrectomy: A Case Report
by Melissa M. Beitner, MBBS; Jonathan Cohen, MD; and Marina S. Kurian, MD
Dr. Kurian and Dr. Beitner are from the Department of Surgery, NYU Langone Medical Center, New York, New York. Dr Cohen is from the Department of Medicine, Division of Gastroenterology, NYU Langone Medical Center, New York, New York.
FUNDING: No funding was provided.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
Bariatric Times. 2012;9(2):22–24
ABSTRACT
Leaks after laparoscopic sleeve gastrectomy can be challenging to manage. Nonoperative management is preferred after the immediate postoperative period. No single treatment is effective in all cases. The best approach is to be persistent, to utilize a multidisciplinary team and to apply one or more endoscopic therapies, often in combination. We present a case of persistent leak after laparoscopic sleeve gastrectomy that highlights these issues.
INTRODUCTION
Staple line leaks after laparoscopic sleeve gastrectomy (SG) are associated with significant morbidity and even mortality. The reported incidence of leaks ranges from 0.5 to 5 percent.[1] In a systematic review of 24 studies with 1,749 patients, the incidence of leak was reported at an average of 2.7 percent.[2] Leak rates greater than 10 percent have been reported with revisional procedures.[3]
The clinical presentation of leaks ranges from asymptomatic radiographic findings to abdominal pain, peritonitis, and sepsis. Thus, a high index of suspicion is warranted.
Early leaks (those detected within a few days of surgery) may be amenable to primary surgical repair, but for late or persistent leaks, a nonoperative approach is preferred. A multidisciplinary team should be employed, utilizing one or a combination of open or percutaneous drainage of intra-abdominal collections, endoscopic clips, fibrin sealants, and self-expandable intraluminal stents.
Here, we present the case of a patient who developed a persistent leak and gastrocutaneous fistula after SG and was successfully managed with a combination of the aforementioned therapies.
Case report and management
A 36-year-old man with a history of obstructive sleep apnea (OSA) and morbid obesity (body mass index [BMI] 40.38kg/m2) underwent laparoscopic sleeve gastrectomy at an outside institution. The greater curve vessels were divided first and then the sleeve gastrectomy was started 5cm from the pylorus. The sleeve was created over a 40cm bougie. The staple line was buttressed with Seamguard (W.L. Gore and Associates, Inc, Flagstaff, Arizona) and the crossing staple lines were reinforced with 2-0 Vicryl sutures. An intraoperative methylene blue leak test was negative. A routine upper gastrointestinal (UGI) contrast series on Postoperative Day (POD) 1 showed a leak, and the patient returned to the operating room. Laparoscopic suture of a 1cm defect in the proximal staple line with debridement of the Seamguard, drainage of the intra-abdominal collection, and placement of a jejunal feeding tube were performed. Nutritional support, antibiotic therapy, and a proton pump inhibitor were instituted. A subsequent UGI series on POD 9 showed no further evidence of leak or obstruction. The patient then developed a left-sided pleural effusion that required drainage on POD 11 because of shortness of breath and a lowered oxygen saturation. On POD 13, the patient became febrile and tachycardic. Contrast-enhanced computed tomography (CT) of the abdomen and pelvis revealed ongoing leak from the gastric sleeve and a fluid collection in the left upper quadrant. Therefore, the patient again returned to the operating room for diagnostic laparoscopy, lysis of adhesions, aspiration of the abscess cavity, and placement of drains. A UGI series on POD 26 showed a small recurrent leak from the proximal suture line of the sleeve. Radiological drainage of an intra-abdominal collection was performed on POD 44 with a drainage catheter left in situ. Subsequent CT scans of the abdomen and pelvis on POD 50 and 63 to evaluate the abscess showed no discrete collection. However, the lateral left portal vein was thrombosed. The patient was placed on warfarin and discharged from hospital on POD 67.
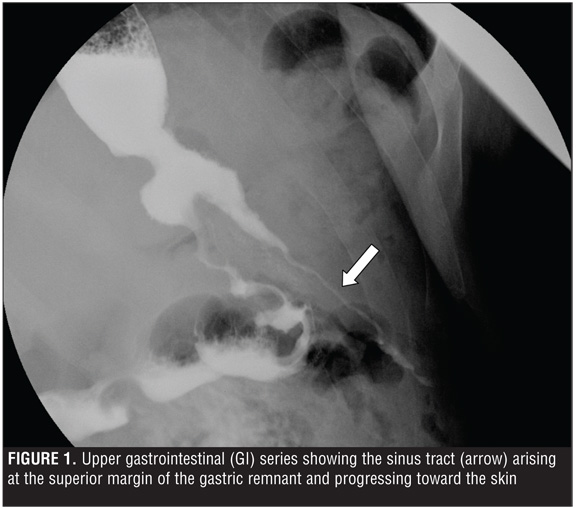
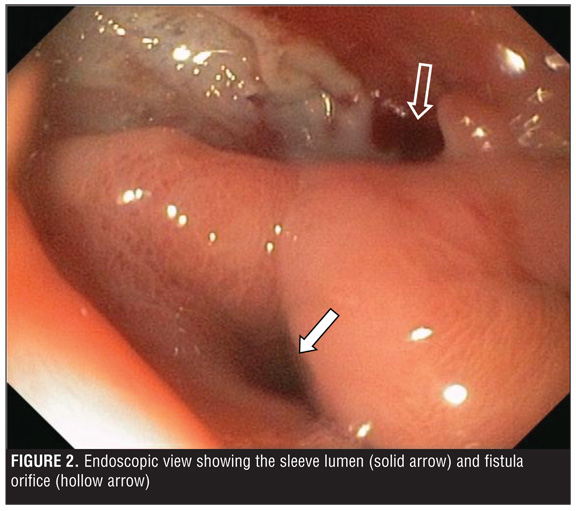
The leak continued to drain via a Jackson-Pratt (JP) drain with no pooling outside the drain on UGI contrast series. The patient subsequently developed a gastrocutaneous fistula with two tracts in communication with the gastric lumen (Figure 1), and during his outpatient follow up, the JP drain was removed. At this point, patient care was transferred to our practice. It had been five months since his initial surgery and his BMI had dropped from 40.38kg/m2 to 28.5kg/m2. We began management of the case by increasing his jejunal tube protein intake from 50g to 100g per day. The patient then underwent endoscopy with injection of 10mL of Tisseel (Baxter, Deerfield, Illinois) fibrin glue into the fistula tract. The tract had a 4mm wide opening and was located at an oblique angle in the dependent portion of a small pouch at the proximal aspect of the staple line below the gastroesophageal (GE) junction and above the sleeve (Figure 2
). The UGI contrast two weeks later showed no further leak and so the patient commenced a liquid diet.
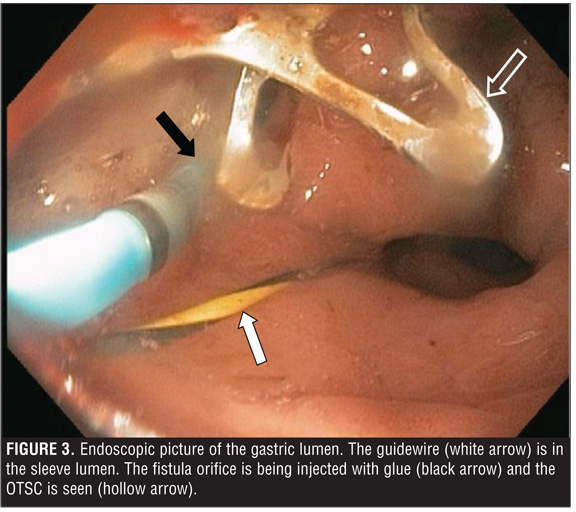
In the weeks following this, the patient presented with recurrent drainage from the gastrocutaneous fistula. This time the UGI contrast showed only one tract and so a second attempt at gluing was made. The tract remained patent. Endoscopic clip closure (of the leak) using an over-the-scope clip (OTSC) (Ovesco Endoscopy USA, Inc, Los Gatos, California) and dilation of the gastric sleeve to 18.5mm (using a 15-16.5-18mm x 180cm CRE balloon dilator [Boston Scientific, Natick, Massachusetts]) was attempted on two occasions as the patient declined stent placement (Figure 3
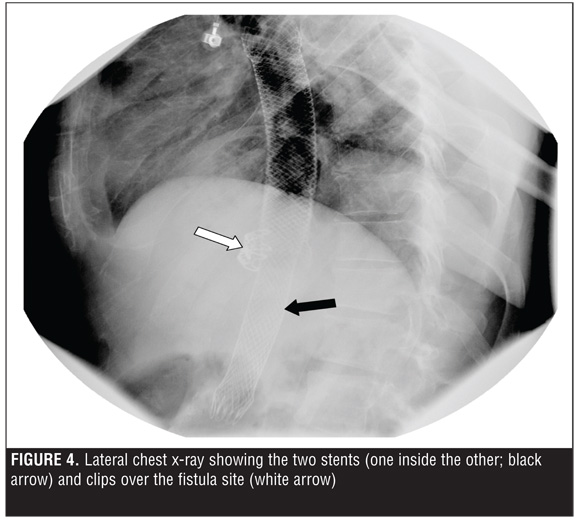
). During one attempt, the angulation of the tract orifice and its location in the dependent portion of a wider outpouching of mucosa impeded successful grasping of both sides of the tract and retraction into the cap on the tip of the scope prior to clip deployment. The tract persisted on UGI contrast series and was identified on endoscopy between the two clips in the area below the GE junction. The fistula tract was again injected with fibrin glue and a fully covered self-expanding metal stent (SEMS, Wallflex stent, Boston Scientific, Natick, Massachusetts]) was deployed. The mouth of fistula was mid-stent, and stent removal was planned in eight weeks. The patient experienced significant heartburn, nausea, and retching. On follow-up esophagram two weeks later, the length of the sinus tract was significantly reduced but the stent had migrated proximally. Therefore, a second SEMS was deployed. A partly covered Wallflex was utilized with the hope that the partly uncovered ends would help prevent migration. The proximal end of the second stent was located in the middle of the first stent and the distal end of the sleeve. As the uncovered proximal end was still within the lumen of the first fully covered stent, it was felt that removability of this second stent would not pose a problem. The area of the fistula, which was clearly demarcated by the metal clips, was tightly sealed in a position in the middle of the serial stent configuration (Figure 4
). The proximal end of the initial stent remained at 30cm from the incisors.
Following the second SEMS deployment, the fistula drainage stopped abruptly. The patient presented four weeks later with epigastric pain and vomiting. An esophagram showed proximal migration of the second SEMS; however, the tract had completely resolved (Figure 5
). The two stents were successfully removed together endoscopically as an outpatient after a total of eight weeks. His course post-stent removal was uneventful and he resumed an oral diet without clinical evidence of recurrent leak.
Discussion
Gastric leaks following SG present a complex management challenge. The widely held definition of an anastomotic leak is that proposed by the United Kingdom Surgical Infection Study Group: “the leak of luminal contents from a surgical join between two hollow viscera” or an outflow of gastrointestinal content through a suture line around an organ.[4] Leaks may be early (within 4 days of surgery), intermediate (between POD 5 and 9), or late (>10 days post operation).[4–6] They may also be classified as type I, those that are subclinical without evidence of dissemination, and type II, those that present clinically and show evidence of dissemination.[4,5] Leaks tend to occur at the GE junction.[7] According to Marquez et al,[4] leaks are more likely to occur in this area due to high intraluminal pressures and low compliance of the gastric sleeve, thus patients with distal stenosis are at greater risk. The pathogenesis of leaks is believed to be related to local ischemia near the staple line subsequent to the use of electrocautery in combination with higher intraluminal pressures postoperatively, rather than staple line dehiscence.[5,6] Baker et al[8] describe the etiology of leaks as being either mechanical/tissue causes or ischemic causes. Classic ischemic leaks occur 5 to 7 days postoperatively when wound healing is between inflammatory and fibrosis phases. These are less frequent. Thus, the majority of leaks are mechanical. This explains the variety of reinforcement techniques and materials available to attempt to reduce leak risk. Unfortunately, as a review by Chen et al[9] of 12 studies of 1589 SG cases shows, reinforcement of the staple line does not necessarily reduce leak rates.
Leaks can be asymptomatic but most commonly present with tachycardia.[10] In a series of 200 SG patients with a three-percent leak rate, Casella et al[11] report the most frequent symptoms to be abdominal pain, fever, vomiting, and dyspnea.
Diagnosis is made on imaging, with CT as the preferred imaging modality for diagnosis and UGI contrast series preferred for surveillance and for determining the origin of the leak;[12] however, CT may be unreliable in patients with a BMI greater than 50kg/m2.[13]
The basic tenets of management include nutritional support with correction of electrolyte imbalances, suppression of gastrointestinal secretions, bowel rest and elimination of downstream resistance, drainage of intra-abdominal collections, and infection and sepsis control. In the case of a gastrocutaneous fistula, skin protection around the external orifice of the fistula must also be considered. The management approach depends on timing of the leak; the tissue becomes inflamed as time from primary operation increases. This decreases the efficacy of both surgical repair and application of endoscopic clips.[14,15] There are several case series in the endoscopic literature using various clips, coagulation, tissue sealants, endoscopically placed sutures, and temporary covered stents either alone or in combination.[16–22]
This case illustrates the fact that multiple endoscopic modalities are often required, and that successful management may require repeated procedures. Prior to endoscopic intervention, the fistula tract should be mapped endoscopically and fluoroscopically, collections drained, and the intragastric mouth of the fistula debrided. Multiple endoscopic therapies might be considered in tandem or in combination. As attempts to seal or close the fistula may not work alone, as this case illustrates, strong consideration to diverting all secretions from the site using removable SEMS should be initially entertained.
Nonoperative management of a chronic fistula after laparoscopic SG requires a multimodal approach, persistence, and a range of endoscopic therapies. The bulk of the literature on endoscopic management of leaks after sleeve gastrectomy and other bariatric procedures comprises small case series in which a number of endoscopic therapies are used often in combination. There is currently no evidence-based algorithm for the treatment of leaks, including guidance as to which modality to try first. The literature does support the notion that treating physicians should be capable of offering the full range of available modalities. In the authors’ opinion, since multiple techniques are often required, strong consideration of using an initial combination of modalities appears reasonable for all but very small diameter fistulae.
Original Lap Band * 9/30/2005 * 4cc 10cm band*, lost 130 pounds. 7 Great years!
Revision surgery to AP small lap band *11/13/2012*, due to large hiatal hernia. I am hopeful about continuing my band journey uneventful and successful. I loved what my old band did for me and I am looking forward for my new band to Keep my weight down![]()

on 5/1/13 11:58 pm
Your welcome, good to see your beautiful face again.
Original Lap Band * 9/30/2005 * 4cc 10cm band*, lost 130 pounds. 7 Great years!
Revision surgery to AP small lap band *11/13/2012*, due to large hiatal hernia. I am hopeful about continuing my band journey uneventful and successful. I loved what my old band did for me and I am looking forward for my new band to Keep my weight down![]()
NYU is Pro, Pro, Pro band but even now when they advertise in the NYC newspapers it is for Sleeves. Dr. Kurian is a sweetheart but she left the Lenox Hill practice with Dr. Roslin for NYU years back - they are still very great friends. At the NYU practice it is unusual to see your surgeon post-op. Usually some other medical staff does your follow-up care. The doc who has his LB there fills and unfills his band when he desires. The staff there has also gotten into training for facial fillers as that is "in demand" when we lose weight (I remember being desperate for fillers for my laugh lines when I was down over 100lbs - Jennifer Hudson has them now and I think they look great but I couldn't see past mine bcuz I never had them at all!). Anyways, I hate to say that it is about the $ there. Actually they are with INAMED or whoever owns the LB. Quite a number of "famous people" have been banded there and publish about it.
God, I sure hope I don't get sick from eating unwashed grapes ![]() . I do this all the time
. I do this all the time ![]() WTH. My office is so close to clean running water!
WTH. My office is so close to clean running water!
Yeah, the stapleline is scarey. I hope mine don't burst. At first I kept being surprised that I could actually eat and the food didn't come directly out of my stomach ![]() . . . I swear this is true. That was my main concern. If it does, I totally trust God. It will be my time and I will die from stomach content flowing through my stomach. Spontanious combustion - is that what they call it. My death! I'd still be glad to have taken a chance because having my big old stomach reduced is grand
. . . I swear this is true. That was my main concern. If it does, I totally trust God. It will be my time and I will die from stomach content flowing through my stomach. Spontanious combustion - is that what they call it. My death! I'd still be glad to have taken a chance because having my big old stomach reduced is grand  . Praise God, I have no adverse effects. Well, I'm still a bit of a chubster because I can eat everything. I never ever get hungry yet I have the most profound everlasting crush on food - that would require brain transplantation. Whatever, I work on it each and every single day. Still hoping to at least bevery close to my goal at my 2 year next month.
. Praise God, I have no adverse effects. Well, I'm still a bit of a chubster because I can eat everything. I never ever get hungry yet I have the most profound everlasting crush on food - that would require brain transplantation. Whatever, I work on it each and every single day. Still hoping to at least bevery close to my goal at my 2 year next month.
Hope you are well and that your band will work forever (I mean this! I don't want to see anyone hurt or fail).
Best,
Layla

3/30/2005 Lap Band installed 12/20/2010 Lap Band REMOVED
6/6/2011 Vertical SLEEVE Gastrectomy
on 5/2/13 11:47 pm
Hey Layla,
Glad to hear you and your Sleeve is doing great, I've always want you and Melly my favorite Band to Sleevers to do well. You had a good surgeon to do your Sleeve.
I think if I had never had weight loss surgery and was seeking it TODAY, I may opt for the Sleeve, but since I have this band, I am not sure if the Sleeve would be effective for me since they are both "restrictive" and but I also fear "dumping syndrome" I've seen what that can do to a person over the years.
My older sister had the VBG "stomach stapling" surgery back in the early 80's so she is close to 30 years post op, she had it very young, and my fear with the Sleeve, I would experience the same thing, (since the Sleeve stapes the stomach) she lost ALL her weight very quickly I remember and she ate "junk food" cheese puffs, etc, there were no follow-ups back then or nutritional counseling.
I watched my sister have "stomach pains and issues for years" she vomited every single day, it was strange though, it was not like a bandsters PB, she did not get food stuck or slime, she would eat her meals and then about 1 hour later she had to vomit, and this was every time I was around her, and it annoyed me to say the least, and my fear of any type of "stomach stapling whether gastric bypass or Sleeve, scares me honestly.
My sister also have dumping like syndrome and she STILL have dumping after all these years after her stomach stapling, I believe it may be hypoglycemia, and she told me that I would not be able to handle it, because it's horrible, you get the shakes, vomiting, sweats, dizzy and feel faint after she eat certain foods, I think if you have any type of stomach stapling surgery whether it be Gastric Bypass, Sleeve or the old Stomach stapling procedure it causes some type of hypoglycemia or "dumping like syndrome" of course gastric bypass is worse when it occurs.
She had to eventually get some of her stomach removed due to ulcers over the years and she had a revision surgery back in 2006 and they put some type of ring around her stomach and the surgeon "tighten it up" but it was a disaster and liked to killed her, she was sick for at least a year after her stomach stapling was revised and she did not lose but about 20 pounds as sick as she was, and she eventually gained that back.
Also, I had two cousins that had Gastric bypass back in the early 80's and they are still fat, so as you can see I am not quick to do anything other than the lap band from what I've personally seen what happens after Gastric Bypass and Stomach stapling wls long term.
I think the Sleeve is a good surgery, you lose quicker than the band, I think virgins Sleevers are probably better than Band to Sleeve revision due to the metabolic factor, but there have been a few that have done well with Band to Sleeve revision.
I wish I had a crystal ball to see how my outcome would be if I revised to the Sleeve, but I am just too scared since you can't turn back, this new band of mine is not like the old one, it's not as restrictive, but that's ok, I just need some help and get my butt back to walking 1-2 hours a day because ultimately -- it does not matter which surgery we pick we will have to change out lifestyle long term for sustained weight loss.
Good luck to you.
Original Lap Band * 9/30/2005 * 4cc 10cm band*, lost 130 pounds. 7 Great years!
Revision surgery to AP small lap band *11/13/2012*, due to large hiatal hernia. I am hopeful about continuing my band journey uneventful and successful. I loved what my old band did for me and I am looking forward for my new band to Keep my weight down![]()

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Thanks for the well wishes! I appreciate it.
I think that your assumption that a virgin sleever will do better than a revision is partially correct. I know it is in MY case. After 4 years of WLS, my motivation is not what it once was, and my metabolism isn't either. However, some revisions do quite well.
Even though they are both restrictive surgeries, they feel very different. With my sleeve, I don't even feel like food is being restricted, it's just that I feel full after eating a small amount. In other words, with the band, I felt my food in my pouch, and new I couldn't take another bite. With my sleeve, I feel like I did before WLS. I just feel full, and I stop eating. It's nice. I can only eat about 2-3 ounces of meat before that happens. Sliders I can eat a bit more of, but not as much as I could with my band. The capacity even with slider foods is limited.
While I know some sleevers that have had dumping experiences, I have luckily never had to deal with it. I can eat anything I want (which is the problem sometimes ha ha) and live normally. Hope you and your new band have a long successful time together! I too, need to get back to exercising!

LapBand Surgery 01/10/08, Revison to Sleeve 04/03/12
![]()
on 5/10/13 12:53 am
Melly, good to hear you Sleeve is a better fit than the band was for you, but you know I've never had a problem getting food stuck with my old band over 7 years, I've been stuck a few times and it was not pleasant, but it was so rare that it never affected my day to day life with my old band.
With my new band I have not yet slimed or PB'd yet, I guess my new band is not that tight yet, and I really don't want it tight, I'd like to hold on to this new band as long as I can and I don't want to damage it by getting it too tight, I've been there and done that.
Original Lap Band * 9/30/2005 * 4cc 10cm band*, lost 130 pounds. 7 Great years!
Revision surgery to AP small lap band *11/13/2012*, due to large hiatal hernia. I am hopeful about continuing my band journey uneventful and successful. I loved what my old band did for me and I am looking forward for my new band to Keep my weight down![]()
My 29 year old daughter is Post Op 3 1/2 months and has spent a total of 35 days total in the hospital. I am so glad to read this. I find very little negativity about the sleeve. We didn't even know what a LEAK was! The weight loss doctor was much more concerned and informative about nutrition. Nutrition is very important but if you have a leak or an abcess, the nutrition is the last thing you are thinking about. It all started the night after outpatient surgery. She was prescribed Xarelto. Instructions were to give daily. She was bleeding terrible from her wound. I called the doc and he said he would see her in the morning. She was in EXTREME PAIN. He saw her the next day on the 4 hour ride home and said to skip one day of Xarelto then start again. 3 days post op she almost died of internal bleeding!! It was so awful!! We went to local ER who rushed her by ambulance to a large hospital an hour away. Their is NO antidote for Xarelto. We didn't know any of this at the time. We were just following doctors orders. When she was discharged for the internal bleeding for 1 week she was back in the hospital with an infected hematoma. She has also had 3 leaks and pleural effusion on lung. She has been on TPN and feeding tube. We are here again getting the second stent. Stents are extremely painful!! I have heard so many success stories but people need to know the dangers and signs of complications. We have a very supportive family and we will get through this. Thank you for the post about leaks.
on 12/22/16 12:27 pm
I'm sorry she is suffering and hope she heals quickly.
I'm curious who her surgeon was, and how experienced they are and what their record is. I'm surprised they gave her xarelto with a freshly cut up stomach. Leaks can happen, but you are (or certainly should have been) leak tested before ever leaving the hospital post op. Xarelto is counter indicated for many stomach and intestinal issues, and if I were you, I'd consult with a medical professional that is not associated with that surgeon.
FluffyPuff · 2 replies · 1052 views

Member Services · 0 replies · 876 views

